

Your thyroid hormone levels are low.
You’re exhausted. Recovery has slowed. Your workouts suddenly feel harder than they should, and you’re cold more often than everyone else around you.
The obvious conclusion?
Your thyroid must be failing.
Not necessarily.
In Part 1 of this series, we explored Hashimoto’s thyroiditis—an autoimmune disease in which the thyroid gland gradually loses its ability to produce thyroid hormone. But there is another form of hypothyroidism that is remarkably common in female athletes, particularly those with persistent low energy availability (LEA) or Relative Energy Deficiency in Sport (RED-S).
In this situation, the thyroid gland isn’t diseased or under attack by the immune system. Instead, the entire hypothalamic-pituitary-thyroid (HPT) axis adapts to chronic energy deficiency by intentionally reducing thyroid hormone production. The result is a hypothyroid state—but one that reflects a coordinated survival response rather than thyroid gland failure.
Understanding that distinction changes everything.
Your Body Is Built to Adapt
One of the most remarkable features of human physiology is its ability to prioritize survival.
When energy intake consistently fails to match the demands of training, the brain begins making difficult decisions about where calories should—and shouldn’t—be spent. Processes that are essential for immediate survival continue, while those that require substantial energy but are not immediately necessary begin to slow.
You’ve seen this adaptation before.
The reproductive system suppresses ovulation, leading to menstrual irregularities or amenorrhea. Bone remodeling slows, resting metabolic rate declines, and the thyroid axis responds in exactly the same way. Rather than maintaining a high metabolic rate, the brain deliberately reduces thyroid hormone production to conserve energy.
This isn’t a mistake—it’s an adaptation.
Why Thyroid Hormone Falls
Triiodothyronine (T3) is the body’s most metabolically active thyroid hormone. It helps regulate resting metabolic rate, mitochondrial function, heat production, skeletal muscle adaptation, protein turnover, and exercise performance.
When energy becomes scarce, maintaining high T3 concentrations is metabolically expensive. Instead, the body lowers T3 production, reducing energy expenditure and allowing available calories to be directed toward vital organs.
Researchers often refer to this physiology as low-T3 syndrome, non-thyroidal illness syndrome, or euthyroid sick syndrome. In female athletes, it represents an adaptive endocrine response to prolonged energy deficiency rather than an intrinsic disease of the thyroid gland.
The goal isn’t to maximize performance.
The goal is survival.
Why Athletes Feel the Difference
Although this adaptation is protective, it comes at a cost.
Reduced thyroid hormone availability slows many of the physiologic processes that athletes depend upon.
Women may notice:
Persistent fatigue
Reduced exercise tolerance
Slower recovery between workouts
Feeling unusually cold
Declining endurance
Reduced training capacity
Difficulty maintaining previous performance
Abnormal menstrual cycles, including infrequent or absent periods
At the cellular level, thyroid hormones act as permissive regulators of skeletal muscle adaptation. They support mitochondrial function, muscle protein turnover, and the metabolic remodeling required for training adaptations. When thyroid hormone availability decreases, these processes become less efficient—not because the body is malfunctioning, but because it is intentionally conserving energy.
Many athletes describe this simply as feeling “flat.” The body has shifted from optimizing performance to preserving energy.
The Misdiagnosis Trap
This distinction becomes critically important in clinical practice.
A female athlete presents with fatigue and declining performance. Laboratory testing reveals a low T3 concentration, and the immediate assumption is often hypothyroidism.
Before concluding that the thyroid gland is failing, however, clinicians must ask a more important question:
Why is thyroid hormone low?
In Hashimoto’s thyroiditis, the thyroid gland cannot produce adequate hormone because autoimmune inflammation progressively destroys normal thyroid tissue.
In low energy availability, the thyroid gland is structurally normal. The brain is simply asking it to produce less hormone as part of a coordinated effort to conserve energy. Although the laboratory findings may appear similar, the underlying physiology is fundamentally different—and different physiology requires different treatment.
Why Thyroid Hormone Replacement Isn’t the Answer
One of the greatest pitfalls is treating adaptive hypothyroidism with progressively higher doses of thyroid hormone while failing to address the underlying energy deficit.
If inadequate fueling persists, the body continues signaling that energy must be conserved. Replacing thyroid hormone alone does not correct the physiologic stress driving the adaptation and may expose athletes to unintended consequences, including accelerated bone loss and an increased risk of stress fractures—particularly concerning in women who may already have compromised bone health from RED-S.
The goal is not simply to normalize laboratory values. It is to restore adequate energy availability.
Hashimoto’s vs. Adaptive Hypothyroidism
Although both conditions result in reduced thyroid hormone availability, they arise for entirely different reasons.
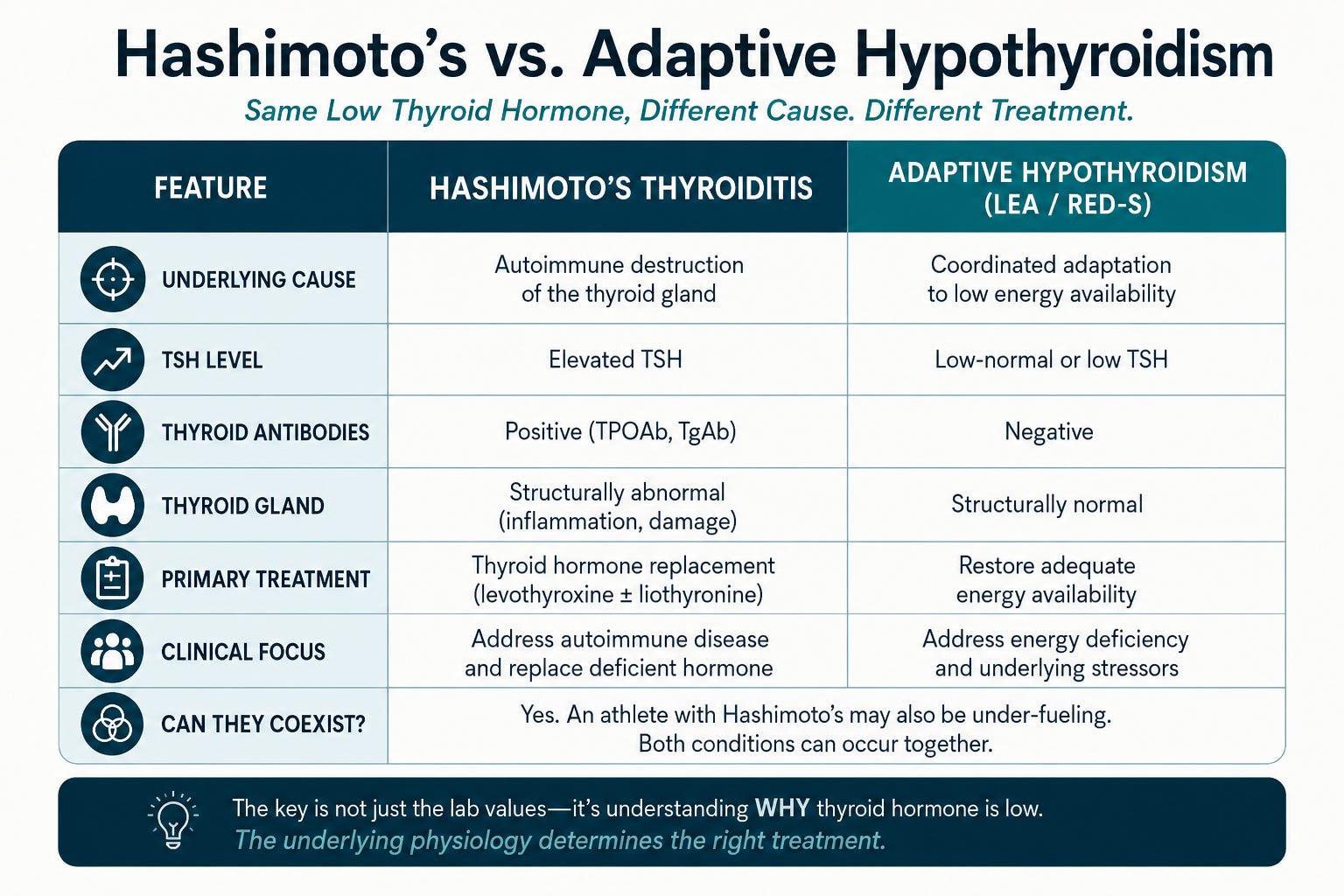
Importantly, these conditions are not mutually exclusive.
An athlete with Hashimoto’s may also be under-fueling. When this occurs, autoimmune hypothyroidism and adaptive suppression of the thyroid axis coexist, there can be even more significant implications for immune function, performance, and overall health.
The Bigger Picture
This concept extends well beyond the thyroid.
Low energy availability doesn’t selectively affect one hormone. It reshapes the entire endocrine system.
The reproductive axis suppresses ovulation. The thyroid axis lowers metabolic rate. Stress hormones rise. Bone metabolism slows. Viewed individually, these hormonal changes appear abnormal. Viewed together, they tell a remarkably coherent story.
The body is adapting.
Key Insights
Low thyroid hormone does not always indicate thyroid gland disease.
In female athletes, chronic low energy availability can produce an adaptive hypothyroid state that conserves energy.
The underlying physiology—not simply the laboratory values—determines the appropriate treatment.
Restoring adequate energy availability addresses the root cause of adaptive hypothyroidism and supports long-term health, recovery, and athletic performance.
Your body isn’t working against you.
It’s doing exactly what it evolved to do.
The goal isn’t simply to normalize thyroid hormone levels. The goal is to create an environment where your body no longer needs to conserve energy—and can once again prioritize strength, recovery, performance, and long-term health.
TAKING NEW PATIENTS!
If you are an active woman or competitive midlife athlete who feels abandoned by mainstream medicine, I’m here for you!
")
It’s time that Women’s Healthcare caught up to the trailblazing generation of active, athletic, and high-performing midlife females!
My telehealth consultation practice does exactly that by focusing on the Reproductive Endocrine needs and Menopausal Care for active, athletic, and high-performing women.
Active and athletic midlife women have needs and risk profiles that are different from the general population. These needs often go unmet by the mainstream medical community due to a lack of understanding of fitness and sport and their impact on mid-life hormonal physiology or even a lack of acknowledgment that this dynamic exists. We put your health, fitness, and performance at the center of the equation so that you can achieve your healthiest, highest-performing self!
You will find all my service offerings on my website, including a link to my calendar so that you can reserve your place in my schedule!